

Many emergency room patients are discharged without understanding how to care for themselves once they get home, researchers say.
In the past, patients who did not follow discharge instructions were often labeled noncompliant. “Now, it’s being called health illiteracy,” Dr. Coleman said, adding that as many as half of all patients are considered to lack the ability to process and understand basic health information that they need to make decisions.
But the patient is only part of the equation, he continued; doctors are notoriously inept at communicating to patients.
The new study found that people were not aware of what they did not understand, suggesting that simply asking a patient if he understands is not enough.
“We’re good at saying, ‘Here’s the information, any questions?,’ ” Dr. Coleman said, “and the person nods his head, but they don’t get it.”
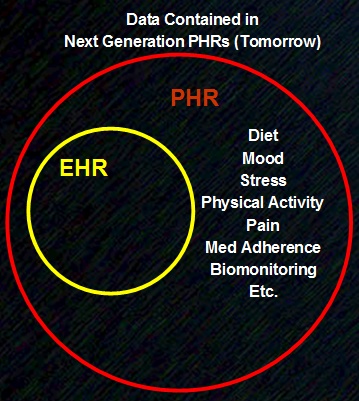
Marina: It all boils down to a lack of information...and ability to transfer information...
